

Author:-Omkar Shirke
The knee is the most common weight bearing joint affected by osteoarthritis (OA), with the disease predominantly affecting the medial compartment of the knee joint . In a typical scenario, If you are experiencing knee pain, you will be ordered to carry out some investigations like MRI or XRAY which shows some structural variations in the knee like a ligament sprain or in worst case a meniscal tear or decreased joint space known as Osteoarthritis (OA), the most feared one.
In a study by Bedson J, he said that “Radiographic knee osteoarthritis is an imprecise guide to the likelihood that knee pain or disability will be present”8. Therefore, we see some people with arthritic changes do not complain of knee pain while some do. OA is nothing but a physiological process and is seen as you age, so it cannot be the diagnosis. If it is not your knee that is causing the pain then what can be the reason behind the pain?
There was another study which said that the spine, hip, and knee are anatomically connected, the pain and discomfort of one joint can have an effect on the other joints naming it as knee-hip-spine syndrome. Thus assuming that the knee pain is caused by problems with the functioning of the knee joint is wrong because in most cases the source of the problem stems from muscle (and accompanying movement) dysfunction or alignment change elsewhere in the body.
In this blog we will be talking about how hip muscle weakness and changes in the pelvic alignment can be the cause of your knee pain.
Omkar Shirke
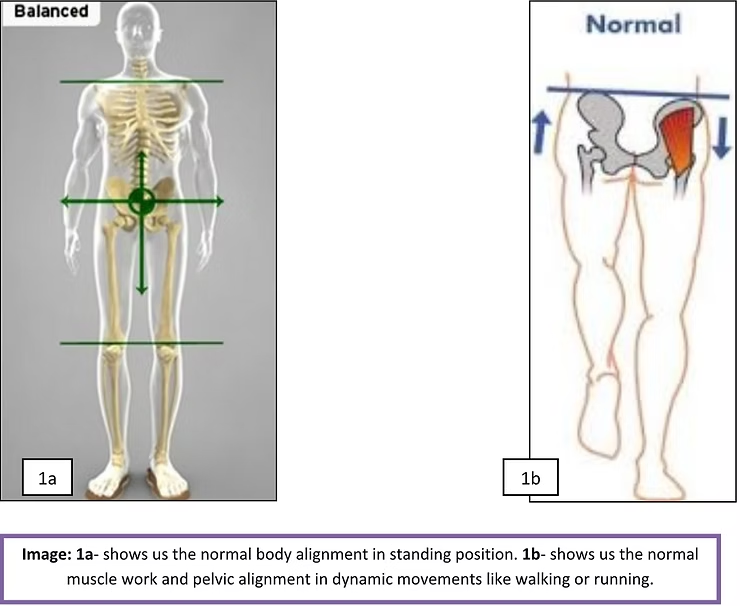
When we are standing or walking (as shown in image 1a and 1b respectively), the weight of our body is absorbed by the discs of our spine and pelvis. This load is then distributed throughout the legs by way of the hip joint, thigh bones (femur), knee joints, leg bones (tibia), ankle joints and finally the feet.
upright body posture is maintained by the alignment of the spine, pelvis, and lower extremities with the support of the muscles around the trunk and hip. Gluteus medius (GMed) is one of the most important muscles around the hip to maintain the pelvic alignment by controlling the pelvic tilting or drop on the leg that is off the ground (swing leg) during dynamic movements like walking and running, thus reducing excessive forces on the knee joint.
What Happens in a Misaligned Pelvis or Weak Hip
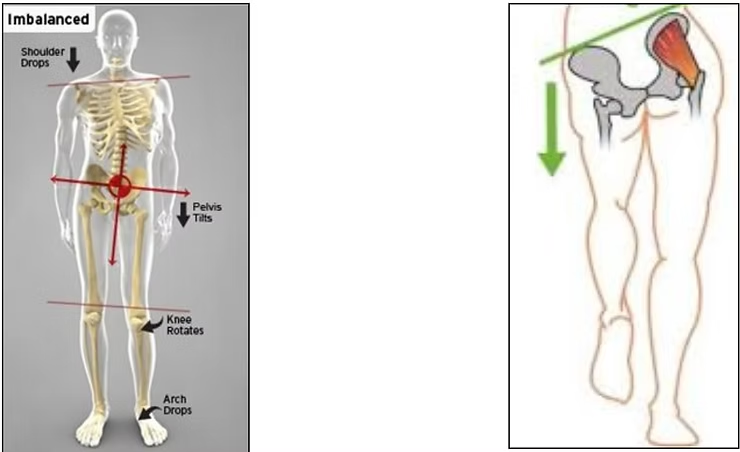
When the pelvis is out of alignment or weak hip muscles, the load of our body weight is distributed into the legs unequally. As a result, any one of the joints in the legs, particularly the knees, can be adversely affected over time, increasing the risk of an acute injury because of the resultant instability in the knee. The knee joint is particularly susceptible to uneven weight distribution because it is a hinge joint, limiting its planes of motion. Additionally, its immediate counterparts in the kinetic chain, the hip and ankle joint, both have greater dimensions in mobility and are better able to tolerate disparate load distribution.
During single leg activities like walking, running, jumping, your foot naturally turns inward, a process called Pronation. When your foot pronates, this starts a chain of events that travels up the leg and creates an inward rotation of the femur (thigh bone). Because the femur is also a part of your knee joint, the movement and control of your femur has a significant effect on your knees. The muscles around the hip joint like Gluteus medius (GMed) and Gluteus maximus (GMax) controls the excessive inward movement of the femur, but when they are weak it directly puts strain on the knee joint.
On the other hand, GMed weakness alone leads to pelvic drop on the swing leg (leg that is off the ground) which is known as Trendelenburg sign and this disturbs the alignment of the pelvis, causing an excessive inward rotation of the thigh, of the leg that is on the ground, putting excessive stress and strain on the tendons, ligament and cartilage, which can lead to a sudden injury or an overuse injury with time.
What are the reasons for Pelvic misalignment or weak hip?
1)Limb length discrepancy: (which means that one leg is short than the other leg).
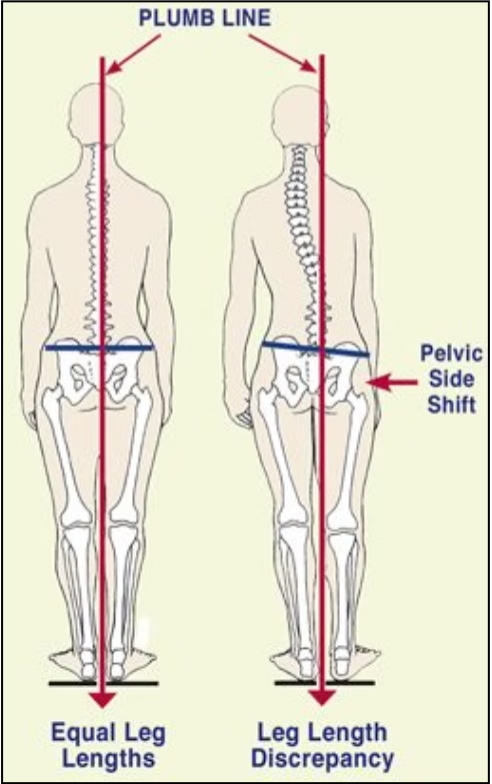
Leg length inequality, defined as the difference in lengths of the two limbs, is very common, occurring in up to 70% of the population5. If the difference is greater than 2cm6 and especially if you are an athlete participating in running activities or your occupation requires extended periods of standing or walking, you are at higher risk for developing knee arthritis in the shorter leg.
2. Prolong awkward postures:
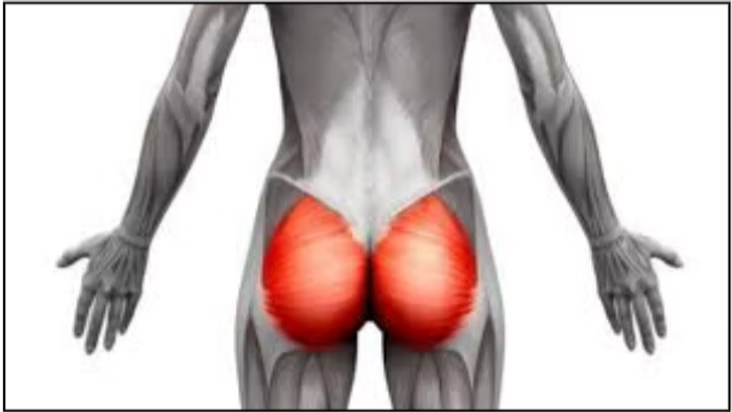
Poor sitting habits at work or poor standing postures can lead to changes in the alignment of your pelvis. Sitting for a long time (more than an hour) causes the Gluteus maximus (GMax) muscle (buttock muscle) to switch off because of lack of activation. As discussed above, this muscle helps control the movements around the knee joint especially in runners. When it is not functioning correctly the movements of the knee become problematic and overtime stressing the joint causing pain.
3. Scoliosis:

It can be congenital (from birth) or functional (due to lifestyle) .This affects the pelvic alignment and over the period of time can leads to osteoarthritis of the knee joint.
4. Hip abductor muscle weakness:
We have already mentioned above the importance of hip abductor muscle that is GMed in maintaining the pelvic alignment and reducing the stresses around the knee joint. Let us now list down the reasons behind weakness of this muscle in some people.

The reasons for hip abductor weakness can be seen in low back pain patients or if you have tight hip adductors. Lifestyle factors can also cause weakness of the GMed. These include the habit of standing with body weight predominantly on one leg with the pelvis swayed sideways and hip joint adducted or of sleeping on one’s side with the top leg flexed and adducted over the other leg7 .These positions potentially weaken the hip abductor muscles, as these muscles remain in a somewhat elongated position (beyond resting physiological length) for sustained periods of time.
5. Trauma-

A slip or fall can also affect the pelvic alignment.
How can a Physiotherapist help you?
If your pelvis is out of alignment, it is to your benefit to get it back and keep it in alignment. Correcting the modifiable risk factors like weak hip muscle and poor posture is often far more cost-effective and has tremendous value in preventing the resultant knee pain. Also, it is said that strengthening the hip abductor and adductor muscles has an influence joint loading and/or OA-related symptoms at the knee joint4.
By working closely with your Physiotherapist, who can examine your posture and pelvic alignment and would guide you with exercises to strengthen your hips, take stress off your knee, and return to your normal activity level quickly and safely.
Think of it this way: It is better to check your car alignment every 3 monthly to help your tires perform properly and avoid them to be worn out early.
Refrences:
Knee–Hip–Spine Syndrome: Improvement in Preoperative Abnormal Posture following Total Knee Arthroplasty. Published 1 July 2019.
Influences of knee osteoarthritis and walking difficulty on knee kinematics and kinetics.
Published in final edited form as: Gait Posture. 2018 March ; 61: 439–444. doi:10.1016/j.gaitpost.2018.01.025.
Ledingham J, Regan M, Jones A, Doherty M. Radiographic patterns and associations of osteoarthritis of the knee in patients referred to hospital. Ann Rheum Dis. 1993;52:520–526. [PMC free article] [PubMed] [Google Scholar].
The effects of hip muscle strengthening on knee load, pain, and function in people with knee osteoarthritis: a protocol for a randomised, single-blind controlled trial.
Kim L Bennell. BMC Musculoskeletal Disorders volume 8, Article number: 121 (2007).
Leg length discrepancy assessment: accuracv and precision in five clinical methods of evaluation*.
Woerman AL, Binder-Macleod SA.
J Orthop Sports Phys Ther. 1984; 5(5):230-9.[PubMed] [Ref list].
Associations of Leg Length Inequality With Prevalent, Incident, And Progressive Knee Osteoarthritis: A Cohort Study.
WF Harvey, Ann Intern Med. 2010 March 2; 152(5): 287–295. doi:10.1059/0003-4819-152-5-201003020-00006.
Bewyer DC and Bewyer KJ. Rationale for treatment of hip abductor pain syndrome. Iowa Orthop J 23:57-60, 2003Cited Here |PubMed
Bedson J, Croft PR. The discordance between clinical and radiographic knee osteoarthritis: a systematic search and summary of the literature. BMC Musculoskelet Disord. 2008;9:116. doi: 10.1186/1471-2474-9-116. [PMC free article] [PubMed] [CrossRef] [Google Scholar].
Knee osteoarthritis prevalence, risk factors, pathogenesis and features: Part I
Behzad Heidari, MD, Caspian J Intern Med. 2011 Spring; 2(2): 205–212
